
Table of Contents
What is Hip Arthritis?
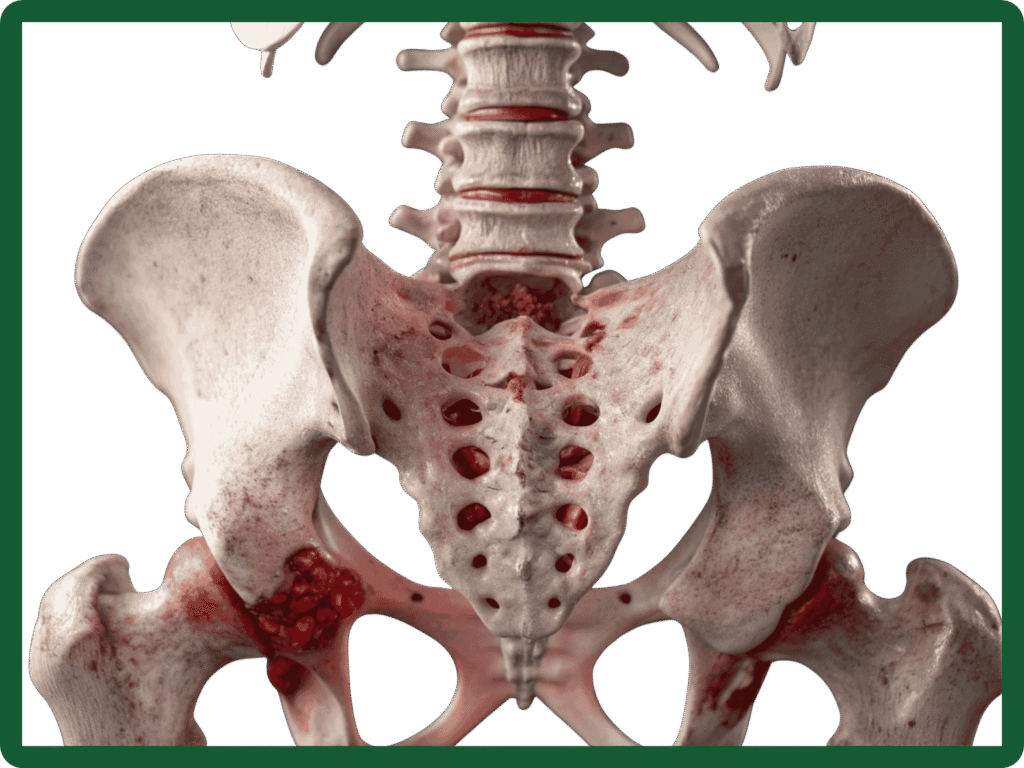
Hip arthritis is the wear-and-tear or inflammation of the hip joint that leads to pain, stiffness and reduced mobility. The hip is a ball-and-socket joint formed by the head of the femur (thigh bone) and the acetabulum (socket) of the pelvis. When the cartilage that cushions the joint wears away, bones rub together, causing pain and limiting everyday activities.
Quick facts
- Most common in people over 50, but can affect younger adults after injury or disease.
- Gradual onset is typical, though symptoms can sometimes follow a fracture or previous hip surgery.
Types of Hip Arthritis
- Osteoarthritis (degenerative): The most common type where cartilage breaks down with age or overuse.
- Rheumatoid arthritis: An autoimmune inflammation affecting multiple joints.
- Post‑traumatic arthritis: Follows fractures or injuries to the hip.
- Avascular necrosis (osteonecrosis): Loss of blood supply to the femoral head leading to collapse and secondary arthritis.
What Causes Knee Arthritis?
- Natural ageing and cartilage wear
- Family history of arthritis
- Previous injuries or fractures
- Carrying extra weight (adds stress to joints)
- Inflammatory conditions (such as rheumatoid arthritis)
- Repetitive movement or high-impact sports
Symptoms & Diagnosis
- Hip or groin pain which often worse with activity and better with rest
- Stiffness in the morning or after sitting
- Reduced range of motion (difficulty putting on shoes, crossing legs)
- Limping or reduced walking distance
- Pain that may refer to the knee or buttock
If symptoms are limiting daily activities or disturbing sleep it’s appropriate to seek specialist advice.
Diagnosis
- Clinical assessment: Detailed history and physical examination looking at range of motion, gait and pain pattern.
- X‑rays: The primary test to assess joint space, bone spurs and deformity.
- Advanced imaging: MRI or CT scans used selectively (for suspected avascular necrosis, unexplained pain, or pre‑surgical planning).
- Blood tests: To rule out inflammatory causes when suspected.
Treatment Options
Treatment options are tailored to your symptoms, age, activity level and imaging findings. Most people start with conservative measures. Surgery is considered when symptoms significantly affect quality of life despite non‑operative care.
- Education & activity modification: Protecting the joint and avoiding painful movements.
- Physiotherapy: Strengthening hip and core muscles, improving mobility and gait.
- Weight loss: Reduces load on the joint and improves outcomes.
- Analgesia and anti‑inflammatories: Tailored to you, taking medical history into account.
- Walking aids: A cane or crutch can ease pain and improve mobility.
- Injections: Corticosteroid injections can offer short‑term relief for flares; other injections (e.g., viscosupplementation, PRP) may be discussed but have variable evidence.
Total hip replacement (THR):
How Hip Surgery Works
Hip replacement surgery involves replacing the worn or damaged parts of the hip with an artificial hip joint. The procedure is performed under either a general or spinal anaesthetic. The duration of surgery is usually between 60–90 minutes. With our enhanced recovery pathway, patients can return home on the day of surgery or within two to three days afterwards.
The common types of hip replacements used are cemented and uncemented. Cement acts like a grout to hold the implant in place, while uncemented implants rely on bony ingrowth for stability. Mr Radja routinely performs a hybrid hip replacement, in which the cup in the pelvic bone is uncemented and the stem in the thigh bone is cemented (as shown in the image above). According to the National Joint Registry (NJR) 2025 annual report, the hybrid hip replacement demonstrates excellent outcomes and long-term survival rates.
Hip Surgery Recovery and Aftercare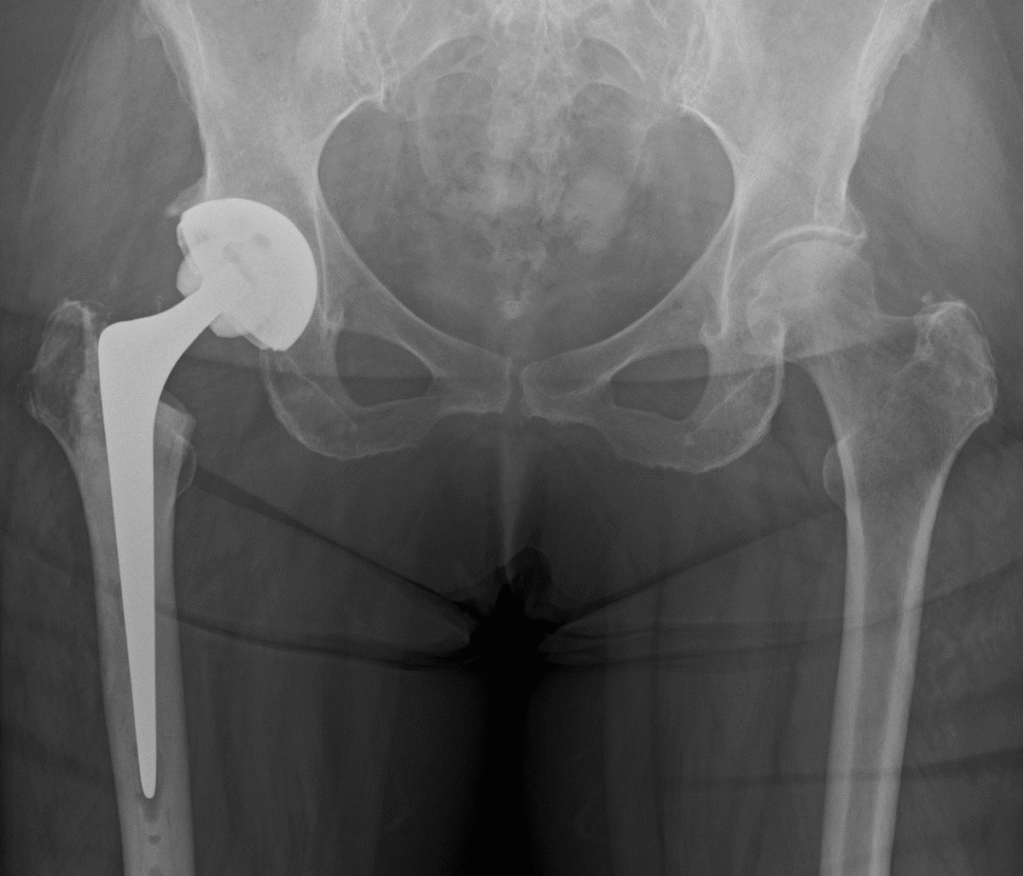
Mr Ellapparadja follows the Enhanced Recovery Pathway (ERP)—a modern, evidence-based approach designed to shorten recovery time after major surgery. ERP significantly reduces hospital stay, with many patients returning home from the same evening of surgery to the following day. His expertise in this pathway is influenced by his training at the Golden Jubilee Hospital in Glasgow, the pioneering centre for ERP practice in the UK.
ERP enables you to be up and walking within a few hours of surgery, supported by physiotherapists. Early mobilisation and an early return home help reduce the risk of deep vein thrombosis and infections, while also improving overall comfort.
Your physiotherapist will provide exercises and instructions on using mobility aids such as crutches or sticks. For the first four to six weeks, you will need these aids to move around, and consistent exercise is essential to ensure your new hip joint functions at its best. The return to normal activities varies between individuals, but most patients are able to resume full activities within three months.
Benefits of Having a Hip Replacement
Total hip replacement has been described as the “operation of the century” for good reason. It can transform your quality of life and allow you to return to the activities you enjoy—free from pain. Recovery speed varies from person to person, but with good physiotherapy and a structured recovery plan, everyday tasks quickly become easier. Activities such as tying shoelaces, getting in and out of a car or bath, walking, and standing typically improve significantly.
Most patients are able to return to hobbies such as golf or gardening with ease within a few months after surgery.
Mr. Radja offers modern techniques including muscle‑sparing approaches and robotic-assisted implantation where appropriate, which may improve precision and early recovery.
What to expect after hip replacement
- Day 0–1: Mobilise with physiotherapy; most patients start walking with aids.
- Weeks 1–6: Pain falls rapidly; continue physiotherapy to rebuild strength and gait.
- 6–12 weeks: Many return to light work and low‑impact activities.
- 3–6 months: Significant functional improvement and most daily activities achievable.
- 12 months: Full recovery and maximal improvement for most patients.
Recovery varies with age, fitness and the exact procedure performed.
Risks & complications
All procedures carry risks. Common and important ones include infection, blood clots, implant wear or loosening, leg‑length difference and dislocation. We will discuss risks specific to your health and planned procedure during consent.
When should you see a specialist?
Please book a consultation if you have:
- Persistent hip or groin pain that limits daily activities
- Worsening stiffness or reduced walking distance
- Symptoms that do not respond to physiotherapy and medications
A specialist appointment includes a focused assessment and a personalised treatment plan.